Osteopontin Human ELISA

Osteopontin (OPN) also named secreted phosphoprotein-1 (SPP1) and sialoprotein-1, is negatively charged aspartic acid-rich, N-linked glycosylated phosphoprotein composed of 314 amino acid residues. OPN exists in various isoforms as a result of alternative splicing, alternative translation and different posttranslation modifications, which result in different molecular weights ranging from 41 to 75 kDa. OPN has primarily been described as a secreted protein but additional evidence suggested that it can also be found in the cytoplasma and nucleus. This form of intracellular OPN (iOPN) is the result of alternative translation and has biological functions distinct from those of secreted OPN (sOPN). OPN molecule has an arginine-glycine-aspartic acid (RGD) cell binding sequence, a calcium binding site and two heparin binding domains. OPN can be modified by thrombin cleavage which exposes additional cryptic integrin-binding sites. Cells bind OPN via multiple cell surface receptors, including various integrin receptors and CD44.
OPN is highly expressed in bone (osteoclasts and osteoblasts) and also secreted by various cell types including macrophages, activated T lymphocytes, endothelial cells, smooth muscle cells, epithelial cells, inner ear, brain, placenta and mammary glands, decidua and kidney. Secreted OPN is found in various biological fluids including blood, milk, urine, cerebrospinal fluid, synovial fluid and seminal fluid. OPN is involved in both physiological and pathophysiological processes in multiple organs and tissues.
One major physiological function of sOPN is the control of biomineralization. As a member of SIBLING protein family with overall negative charge, OPN is able to directly bind to specific apatite crystal faces thereby acts as a mineralization inhibitor. OPN is also strongly upregulated at sites of ectopic, pathologic calcification – such as vascular calcification, valvular calcification, renal crystal formation and gallstone formation and prevents or limits calcification. Moreover OPN is required for bone remodeling process and stimulates adhesion, migration and bone resorption by osteoclast.
Abundant evidence suggests that OPN plays a critical role in acute inflammation and leukocyte recruitment and in chronic inflammatory diseases such as multiple sclerosis, Crohn´s disease and other autoimmune disorders, several types of cancer and cardiovascular diseases. OPN may exert both pro-inflammatory and anti-inflammatory actions depending on biological requirement. Increased OPN levels in cerebrospinal fluid have been found in patients with inflammatory neurological disease (e.g. multiple sclerosis, Alzheimer´s disease and neuromyelitis optica) and may reflect disease progression.
OPN is a critical regulator of adipose tissue inflammation in obesity. In adipose tissue, OPN is upregulated, induces infiltration and activation of macrophages and these infiltrated macrophages produce proinflammatory cytokines which contribute to adipose tissue insulin resistance and type 2 diabetes. Furthermore, OPN was shown to negatively influence atherosclerosis and hepatic disorders which are strongly associated with obesity and type 2 diabetes such as non-alcoholic fatty liver disease (NAFLD) and diabetic nephropathy. Clinical approaches show that circulating OPN levels in obese patients were elevated compared with lean subjects and were further increased in obese diabetic or insulin resistant patients.
OPN is a tumor-associated antigen that is highly expressed in multiple human cancers including lung cancer, breast cancer, melanoma and mesothelioma. The level of circulating OPN may be indicative of cancer progression, metastasis, and prognosis. Recent study shows, that OPN plasma level of metastatic breast cancer patients is significantly higher in comparison with a non-metastatic group, and OPN can be a biochemical marker giving early signal for metastases.
Urinary OPN concentration can be used for investigation of renal stone disease because OPN inhibits urinary crystallization.
It has been reported that elevated OPN level was presented in plasma and synovial fluid of patients with rheumatoid arthritis (RA) and with osteoarthritis (OA) compared to the control OPN level. Measurements of plasma and synovial fluid levels of OPN in patients with primary knee OA reveal significant correlation with severity of knee pain and radiologic progression of the disease.
Effect of OPN for cell survival was demonstrated on epithelial, endothelial and smooth muscle cells. The experiment indicated that the OPN binding to αvβ3 integrin of endothelial cells activates the pro-survival transcription factor NFκB and protects cells from undergoing apoptosis.
Current clinical investigation of critically ill patients with and without sepsis described that persistently elevated OPN serum concentrations are associated with unfavorable outcome independent of the presence of sepsis. Studies indicate that OPN may be a prognostic biomarker in these patients during early course of treatment in medical intensive care units.
Type
Sandwich ELISA, Biotin-labelled antibody
Applications
Serum, Urine, Cerebrospinal fluid, Milk, Plasma (EDTA, citrate, heparin)
Sample Requirements
Plasma: 10 µl/well – Serum: 20 µl/well
Urine, CSF, Breast milk: 5 µl/well
Osteopontin is proteolytically cleaved by thrombin during blood clotting, thus, serum osteopontin levels are significantly lower than plasma levels. To prevent OPN cleavage in samples during clotting, PMSF can be added.
Samples should be assayed immediately after collection or should be stored at 20°C or preferably at 70°C. Storage of samples at 4°C should be avoided since it leads to a significant decrease in OPN levels.
Storage/Expiration
Store the complete kit at 2 8°C. Under these conditions, the kit is stable until the expiration date (see label on the box).
Calibration Curve
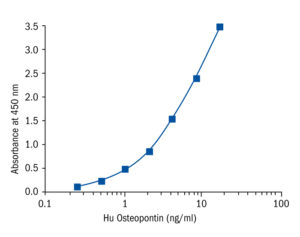
Calibration Range
0.25 – 16 ng/ml
Limit of Detection
87 pg/ml
Intra-assay (Within-Run)
n = 8; CV = 5.7 %
Inter-assay (Run-to-Run)
n = 6; CV = 3.9 %
Spiking Recovery
EDTA Plasma: 97.2 %
Serum: 90.2 %
Dilutation Linearity
EDTA Plasma: 98.7 %
Serum: 99.42 %
- Ahmad R, Al-Mass A, Al-Ghawas D, Shareif N, Zghoul N, Melhem M, Hasan A, Al-Ghimlas F, Dermime S, Behbehani K. Interaction of osteopontin with IL-18 in obese individuals: implications for insulin resistance. PLoS One. 2013;8 (5):e63944
- Bertola A, Deveaux V, Bonnafous S, Rousseau D, Anty R, Wakkach A, Dahman M, Tordjman J, Clement K, McQuaid SE, Frayn KN, Huet PM, Gugenheim J, Lotersztajn S, Le Marchand-Brustel Y, Tran A, Gual P. Elevated expression of osteopontin may be related to adipose tissue macrophage accumulation and liver steatosis in morbid obesity. Diabetes. 2009 Jan;58 (1):125-33
- Braitch M, Nunan R, Niepel G, Edwards LJ, Constantinescu CS. Increased osteopontin levels in the cerebrospinal fluid of patients with multiple sclerosis. Arch Neurol. 2008 May;65 (5):633-5
- Bramwell VH, Doig GS, Tuck AB, Wilson SM, Tonkin KS, Tomiak A, Perera F, Vandenberg TA, Chambers AF. Serial plasma osteopontin levels have prognostic value in metastatic breast cancer. Clin Cancer Res. 2006 Jun 1;12 (11 Pt 1):3337-43
- Cho EH, Cho KH, Lee HA, Kim SW. High serum osteopontin levels are associated with low bone mineral density in postmenopausal women. J Korean Med Sci. 2013 Oct;28 (10):1496-9
- Comi C, Carecchio M, Chiocchetti A, Nicola S, Galimberti D, Fenoglio C, Cappellano G, Monaco F, Scarpini E, Dianzani U. Osteopontin is increased in the cerebrospinal fluid of patients with Alzheimer’s disease and its levels correlate with cognitive decline. J Alzheimers Dis. 2010;19 (4):1143-8
- El-Tanani MK, Campbell FC, Kurisetty V, Jin D, McCann M, Rudland PS. The regulation and role of osteopontin in malignant transformation and cancer. Cytokine Growth Factor Rev. 2006 Dec;17 (6):463-74
- Gao SG, Li KH, Zeng KB, Tu M, Xu M, Lei GH. Elevated osteopontin level of synovial fluid and articular cartilage is associated with disease severity in knee osteoarthritis patients. Osteoarthritis Cartilage. 2010 Jan;18 (1):82-7
- Haider HM, Amin IR, Ahmad KA. Plasma and synovial osteopontin levels, are they associated with disease severity of primary knee osteoarthritis in Egyptian patients?. Egypt Rheumatologist . 2015;37:29-34
- Inoue M, Shinohara ML. Intracellular osteopontin (iOPN) and immunity. Immunol Res. 2011 Apr;49 (1-3):160-72
- Iwadate H, Kobayashi H, Kanno T, Asano T, Saito R, Sato S, Suzuki E, Watanabe H, Ohira H. Plasma osteopontin is correlated with bone resorption markers in rheumatoid arthritis patients. Int J Rheum Dis. 2014 Jan;17 (1):50-6
- Kahles F, Findeisen HM, Bruemmer D. Osteopontin: A novel regulator at the cross roads of inflammation, obesity and diabetes. Mol Metab. 2014 Jul;3 (4):384-93
- Kariya Y, Kariya Y, Saito T, Nishiyama S, Honda T, Tanaka K, Yoshida M, Fujihara K, Hashimoto Y. Increased cerebrospinal fluid osteopontin levels and its involvement in macrophage infiltration in neuromyelitis optica. BBA Clin. 2015 Jun;3:126-34
- Kiefer FW, Zeyda M, Gollinger K, Pfau B, Neuhofer A, Weichhart T, Saemann MD, Geyeregger R, Schlederer M, Kenner L, Stulnig TM. Neutralization of osteopontin inhibits obesity-induced inflammation and insulin resistance. Diabetes. 2010 Apr;59 (4):935-46
- Kiefer FW, Zeyda M, Todoric J, Huber J, Geyeregger R, Weichhart T, Aszmann O, Ludvik B, Silberhumer GR, Prager G, Stulnig TM. Osteopontin expression in human and murine obesity: extensive local up-regulation in adipose tissue but minimal systemic alterations. Endocrinology. 2008 Mar;149 (3):1350-7
- Lund SA, Giachelli CM, Scatena M. The role of osteopontin in inflammatory processes. J Cell Commun Signal. 2009 Dec;3 (3-4):311-22
- Mazzali M, Kipari T, Ophascharoensuk V, Wesson JA, Johnson R, Hughes J. Osteopontin–a molecule for all seasons. QJM. 2002 Jan;95 (1):3-13
- Nassar HR, Namour AE, Shafik HE, El Sayed AS, Kamel SM, Moneer MM, Zakhary NI. Prognostic significance of plasma osteopontin level in breast cancer patients. HeSMO. 2015;6 (1):27-32
- Patouraux S, Bonnafous S, Voican CS, Anty R, Saint-Paul MC, Rosenthal-Allieri MA, Ag